Brisk walking was always considered a good way to reduce blood pressure, but now some researchers have found that regular stretching can be a better method to control hypertension. They have also found that stretching is also beneficial for those who are still at risk of developing high blood pressure.
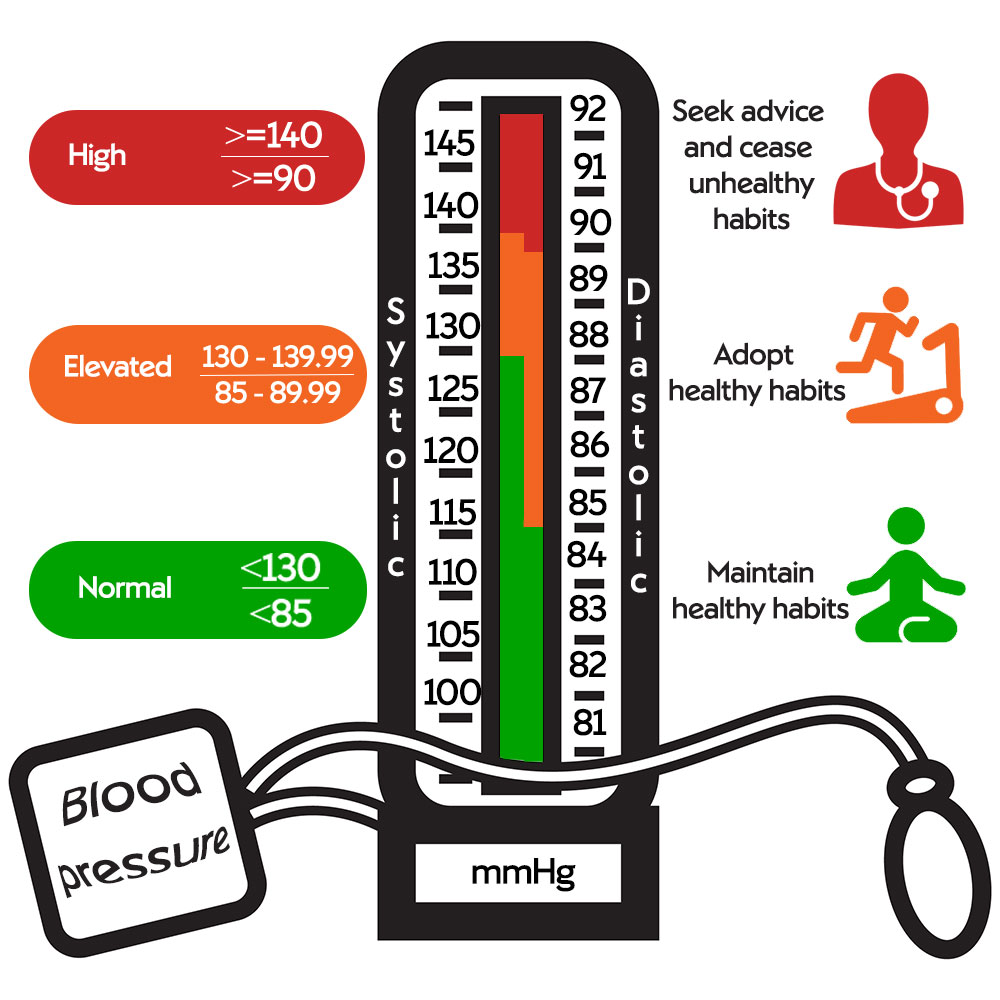
High blood pressure else described as hypertension, is one of the primary risk factors for getting heart – and kidney problems, which can result in fatality.
Therefore it is important to keep your blood pressure within normal levels, and even more important to understand how you can prevent hypertension.
A new study from the University of Saskatchewan (Usask) has found that stretching is more effective in lowering blood pressure than the formerly believed strategy of brisk walking and physical exercise. Participants were asked to do either 30 minutes of brisk walking or 30 minutes of stretching every day for eight weeks. With all the necessary strategies in place to make it a random trial, there was a more significant improvement in the blood pressure levels of those participants that stretched for 8 weeks versus the participants that did brisk walking for 8 weeks.
There are as much as 72 muscles surrounding your hips and upper leg. not even to mention the hordes of muscle structures that builds up from the hips into your back. When it comes to bones, the socket is made of three joined pelvic bones – the ilium, the ischium and the pubis. The hip joint is made up of four bones.
The hip bones, or os coxae, make up part of the pelvic girdle, which connects the lower limbs to the axial skeleton. Each hip bone is a large, flattened, and irregularly shaped fusion of three bones: the ilium, ischium, and pubis.
The pelvis refers to the lower abdominal area, with the main function of this bone structure being protection and support. It protect all the internal soft tissues and organs as well as giving support to the hip joints.
The pelvic floor is like a “mini-trampoline made of firm muscle,Just like a trampoline gymnasts would use, the pelvic floor is flexible and can move up and down with the forces it receives from walking , running and daily activities.
According to the American Association for the Surgery of Trauma, about 8 to 9 percent of blunt trauma includes pelvic injury, Gillogley says. “These accidents include falls, motor vehicle crashes, bicycle accidents, and pedestrians being struck by moving vehicles. With these serious injuries, pelvic bones can fracture or dislocate and sometimes bladder injury even occurs.
How to take care of the Hips?
For prevention of pain and injury keep them MOBILE AND STRONG !
See these exercises on a video from Adarsh Williams
Scientific basis of Active isolated stretching – A research review
Pertti T. Kukkonen
Research Director, Espoo, Finland
ABSTRACT
Kukkonen PT. Scientific Basis of Active Isolated Stretching: A
Review. JEPonline 2019(22)2:58-70. Aaron L. Mattes made the
observation that stretching along the line of stress of the muscle
and relaxation of the muscle in each repetition of stretch would
diminish the resistance to stretching. Based on this observation,
the purpose of this review will be to demonstrate that Active
Isolated Stretching (AIS) is performed with less torque than static
stretches, but nonetheless increases joint range of movement
(ROM) of the hamstring muscles more so than static stretches.
By searching the studies on static stretching, it was possible to
find 14 articles that reported mean maximal torques of hamstring
and calf muscles. These measurements were compared to
optimal – maximal torque of AIS. The result is that the AIS
stretches are performed with less torque than static stretches.
This inference should be confirmed by experimental studies. It
was also possible to find 4 articles that reported AIS increasing
ROM of the hamstring muscles more or at least the same
amount as static stretching. Mattes finding, that stretching along
the line of stress of the muscle and relaxation of muscle in each
repetition is the main mechanism of action of AIS. The findings of
this review would be the basic theory of AIS. The main
mechanism of AIS could renew the stretching techniques.
Hence, this review should have very positive effect on exercise
physiology.
Key Words: Flexibility, Musculoskeletal, Relaxation
59
INTRODUCTION
Few exercise physiology research studies have been published on Active Isolated
Stretching (AIS). The mechanism of action of AIS has not been thoroughly investigated.
On some other stretching techniques, Weppler and Magnusson (31) published in 2010
a review of the mechanisms of action of the techniques. This development was made
possible by evaluating the biomechanical properties of stretching. When including the
use of tension in muscle length evaluation, studies on stretching were able to construct
torque-angle curves before and after stretching. Measuring maximal torques used in
most stretching techniques became possible.
Mattes (20-23) was developing AIS when he was directing Kinesiotherapy Clinics at the
University of Illinois in 1972-1976 and at the University of Toledo in 1976-1979. He is an
expert in massage therapy and kinesiotherapy. As an athlete himself, he was frustrated
when he suffered an injury and there were only ineffective rehabilitation methods
available. By trying a great number of positions and stretches, he finally found a
stretching technique that seemed to function properly. Mattes found in his many trials
the combination of stretching along the stress line of the muscle and relaxation of the
muscle to be stretched in each of the repetitions. Both were needed in order to diminish
the resistance to stretching of a muscle.
If the resistance to stretching is smaller along stress lines, why have the numerous
researchers not discovered, even by accident, to use stress line of muscle when
investigating static stretching? If the muscle is not relaxed, stretching along the stress
line does not diminish the resistance. Relaxation could be a precondition for smaller
resistance.
According to Mattes (21), AIS is performed very lightly, with less than 1 lb (4.5 Nm)
pressure. The optimum pressure is only 6 to 8 ounces or 1.7 to 2.3 Nm (30). Stretch
lasts 1 to 2 sec and there are 8 to 10 reps of stretch. The muscle to be stretched is
relaxed by contracting the antagonist muscle when moving body part actively from the
starting position to the stretching position.
Mattes would have been developing AIS gradually and finally in books of 2000 (20,23)
and 2012 (21) he concluded that the laws of Sherrington and Wolff formed the scientific
basis of AIS (20,21). But, since this was not convincing evidence of the scientific value
of AIS, he tried to get medical researchers involved in developing AIS. According to
“Massage Magazine” (internet), Mattes and his associate, Jeffrey Haggquist DO,
arranged in Washington D.C. in June of 2008 from the 10th to the 14th a seminar,
where AIS and medical experts together developed AIS applications. The aim was also
to encourage researchers to start researching AIS. In 2009, Mattes was working with
NIH (National Institutes of Health) to design pilot studies to demonstrate the value of
AIS to the scientific community (30).
These attempts did not succeed because the researchers at that time did not have the
tools to show the value of AIS. Before the year 2010 only a few research teams were
60
able to use torque-angle curves and maximal torques in stretching and had devices to
measure them. The main interest of these research teams was in sensory theory of
static stretch and not in AIS. Since Weppler and Magnusson`s review article (31) in
2010, torque-angle curves and maximal torques in stretching have been better known.
SOME IDEAS OF AARON L. MATTES
Relaxation
Mattes (21) states that only relaxed myofascial structures can be optimally stretched.
Relaxation is based on Sherrington`s law of reciprocal inhibition. Contraction of an
agonist muscle on one side of a joint sends a signal to the opposite side muscle to
relax. The positions and movements of AIS are designed so that the movement of
stretching a person from a starting position to a stretching position relaxes the muscle or
muscles automatically. Relaxation is augmented by exhaling of the person when moving
through the stretching position. After each stretch, the area being stretched should
always be returned to the starting position before the next repetition. There should be 8
to 10 reps for each stretch.
Stretching Along the Lines of Stress in the Body and Muscle
Stretching should be directed along the stress line for each muscle. Mattes derived this
principle from Wolff`s law that originally concerns bones. Also, the sheets of fascia are
laid down along the lines of stress within the body and they adhere to proper anatomical
positioning. The conclusion by Mattes (21) is supported by Myers (26) who
demonstrated how long collagen molecules of muscle orient themselves along the lines
of tension of the muscle. Mattes (21) expressed the same anatomical feature on macro
level with the collagen fibres laid down along the lines of stress within the body.
Mattes studied origin, insertion, and action of each muscle to decide the optimal
direction it should be stretched. Parts of some muscles have their own stress lines and
optimal stretches. Stretching along the line of stress of the muscle and relaxation of
muscle minimizes tension and friction among fascial sheets so that they start to move,
although stretch is done with minimal pressure or torque. In repetitions of the stretch,
this works to break down adhesions and scar tissue formations that have been caused
by inflammation resulting from soft tissue traumas. Breaking down adhesions mitigates
or removes muscular pain. Stretches also realign collagen fibres and reduce muscle
spasms.
Repetitive Muscle Contractions and Breathing in Their Rhythm
In order to facilitate relaxation, one should exhale when moving from starting position to
stretching position and inhale when returning back to starting position. Breathing and
repetitive muscle contractions deliver greater amounts of circulating blood, oxygen, and
nutrition to the muscles. They also stimulate circulation and drainage of lymph, which
helps to eliminate metabolic wastes, such as lactic acid. Joint angle expands in each
repetition. Combining flexibility and strength training systems is one feature of AIS.
Muscle opposite to the one being stretched is being strengthened at the same time.
This takes place in each repetition. Movement increases strength of muscles in good
61
balance on both sides of the body, as well on both sides of the lower and upper
extremities when all major muscles are stretched systematically.
COMPARISON OF THE MAXIMAL TORQUES IN AIS AND STATIC STRETCHING
Because no studies have been published on the mechanisms of action of AIS in peerreviewed
journals, a Master of Science thesis in kinesiology at the Brock University in
Ontario, Canada, has been used (for one part) in the comparison. The title of the study
is “Active Isolated Stretching: An Investigation of the Mechanical Mechanisms” by
Longo (14). The experimental part of the study provides some valuable hints on the
mechanisms of action of AIS. The subjects in the study were university students (8
females and 2 males) with tight hamstrings. During 6 wks they made daily 2 series of
knee (right side) extension AIS stretches with 10 reps with a 30-sec interval between
series. The stretches were done with less than 1 lb force and the last (10th) repetition
was taken so far that the subject felt a light irritation. The left leg was a control. Before
and after the 6 wks of stretching, knee extension ROM and resistance to stretch were
measured with a dynamometer (Biodex System 3) for both legs (with gravity correction).
The Delsys Bagnoli-4EMG-system was used to monitor electric activity of the vastus
lateralis and hamstring muscle group with electrodes placed on the muscles.
Main result of Longo`s experiment was that the mechanism of action of AIS is not
mechanical. Values measured before and after stretching are approximately on the
same line (Figure 1). Knee extension ROM increased significantly by 15° and there was
an indication that long-term AIS (6 wks in the experiment) would be efficient in
increasing ROM. Longo also made the conclusion that EMG measurements show that
the hamstring muscles were significantly less active than the vastus lateralis muscle
and that reciprocal inhibition was occurring and hamstrings were relaxed (14 p. 67).
Figure 1 is a modified figure from Longo`s study on knee extension AIS-stretching (14).
The person was applying only 30 Nm torque to do the final repetition of knee extension
AIS stretch. Unfortunately, mean maximal torque after stretching for all the 10 subjects
is not available. According to Mattes (30), the optimal AIS stretch is very light, about 2
Nm and with 10 reps at a torque of 20 Nm. The upper limit for the use of force is less
than 1 lb (or 4.5 Nm) torque. Therefore, for AIS optimal – maximal torque range is 20 to
45 Nm for comparison with static stretching.
62
Last column of Table 1 gives a list of mean maximal torques used in static stretches of
hamstring and calf muscles. The first 5 studies are found as references in Weppler and
Magnusson`s review article (30). The rest of the 9 studies are found from a review by
Freitas et al. (6) published in 2018. The review had the restriction in searching of
articles that only stretching interventions of more than 2 wks duration were accepted.
Table 1. A List of Mean Maximal Torques used in Static Stretches.
Studies of Static Stretching Increase Mean Maximal
Stretching Exercise in ROM Torque
weeks degrees Nm
Hamstring Muscles
Magnusson et al. (16) — — 75
Reid and McNair (28) 6 10 114
Ylinen et al. (32) 4 17 105
Ben and Harvey (2) 4 10 65
Folpp et al. (5) 4 9 67
Magnusson et al. (17) 3 10 52
Gajdosik (7) 3 13 50
Law et al. (12) 3 10 44
Chan et al. (4) 4 11 28
LaRoche & Connolly (11) 4 9 149
Calf Muscles
Gajdosik et al. (8) 8 5 122
Guissard & Duchateau (10) 6 8 29
Gajdosik et al. (9) 6 7 26
Blazevich et al. (3) 3 8 110
63
According to the studies in Table 1, mean maximal torques of static stretching range
between 26 and 149 Nm. For AIS the optimal-maximal range of torque would be 20 to
45 Nm. Although there is slight overlap in the ranges in Figure 2, one can infer that with
a quite high probability Figure 2 demonstrates that AIS is performed with less torque
than static stretch. The inference is reasonable, and it can be confirmed by studies
whereby the subjects are performing AIS and static stretches and torque-angle
relationships are measured as well as mean maximal torques after stretching. The
studies should be made both for hamstring muscles and calf muscles using available
measurement devices.
Table 2. Gender of Subjects has an Influence on Mean Maximal Torque.
Studies of Static Mean Maximal Subjects in
Stretching Torque Stretch Group
Nm Males Females
Hamstring Muscles
Magnusson et al. (16) 75 10 0
Reid and McNair (28) 114 23 0
Ylinen et al. (32) 105 12 0
Ben and Harvey (2) 65 9 21
Folpp et al. (5) 67 8 12
Magnusson et al. (17) 52 0 7
Gajdosik (7) 50 12 0
Law et al. (12) 44 15 15
Chan et al. (4) 28 6 4
LaRoche and Connolly (11) 149 9 0
Calf Muscles
Gajdosik et al. (8) 122 0 10
Guissard and Duchateau (10) 29 8 4
Gajdosik et al. (9) 26 0 6
Blazevich et al. (3) 110 12 0
Gender and age seem to influence the results of stretching, mainly because females are
more flexible than males and because flexibility is decreased after a certain age. In the
studies, males and aging subjects seem to use greater maximum torque than females
and younger persons. In the LaRoche and Connolly (11) study, the average age of the 9
participating men was 31 yrs of age, and some of them may have been over 60 yrs of
age. Therefore, they are less flexible and the mean maximal torque is high, 149 Nm.
The other high mean maximal torque of 122 Nm is in the Gajdosik et al. (8) study on calf
muscles of older women with an average age of 73 yrs. A very different story is reported
64
in Chan et al. (4) where the subjects are young women and men with an age range of
18 to 25 yrs and mean maximal torque is only 28 Nm.
THE MECHANISM OF ACTION OF AIS
The main mechanism of action of AIS would be stretching along the lines of stress in
the muscle and relaxation of the muscle to be stretched in each of the 8 to 10 reps.
Mattes and several AIS experts have a 40-yr experience in applying AIS in sport, sport
injuries, and various musculoskeletal problems. This means that there is a large
experience-based knowledge behind the other suggested mechanisms of action of AIS.
As a consequence of the main mechanism, friction among fascial sheets is reduced and
they start to move. This movement among fascial sheets during repetitions breaks down
adhesions and scar tissue formations of muscles. The breaking down of adhesions
mitigates or removes muscular pain. This is the first suggested mechanism, which
should be confirmed by more research in this area.
Breathing and repetitive muscle contractions accelerate circulation of blood and lymph.
This delivers oxygen and nutrition to muscles and reduces metabolic wastes like lactic
acid. The repetitive muscle contractions also work as strength training. These would be
the second suggested mechanism. Again, more research studies is essential to confirm
the suggested mechanisms. There might be other effects of AIS, such as stretching
reducing muscle spasms and realign collagen fibers as Mattes has suggested.
Therefore, the two suggested mechanisms may be just the beginning of the list of
possible mechanisms of AIS action.
ONE ASSUMPTION OF AIS SHOULD BE REVISED
Magnusson (18) review published in 1998 concluded that contractile reflex activity does
not contribute to the response in a slow static stretch. Magnusson`s conclusion is valid
also in regards to AIS. Alter (1) in his “Science of Flexibility” published in 2004 was
strongly critical of the assumption of the stretch reflex in AIS (1 p.164). Taking into
account these critics, the assumption of AIS, that the stretch reflex is activated if the
stretch continues more than 2 sec, should be revised. It could be revised without any
change in the way stretches are made. The change would only affect the way AIS is
justified. It has been demonstrated above that the best justification for AIS is stretching
along the stress lines of body and relaxation of the muscle to be stretched. Even in the
future, AIS-stretches would be performed in 2 sec with low force and by the rhythm of
breathing.
After the revision suggested above there would be no changes in the way AIS stretches
are done. Therefore, experimental studies on the effect of AIS on increasing joint ROM
would need no changes. Nor would there be any changes in the many ways AIS is used
in sports. The warning that one should not stretch more than 2 sec is in fact useless and
incorrect theoretical justification for AIS. To be better approved and appreciated, the
revision is inevitable.
65
WOULD AIS INCREASE JOINT ROM MORE THAN STATIC STRETCHING?
Four studies on this subject were published in peer-reviewed journals. They fulfil the
criteria of a scientific study. The studies have a randomized control group in addition to
the two groups doing the AIS and static stretches. Randomized assignment of the
subjects to the groups was secured. The studies were published as one page abstracts,
which may reflect the somewhat poor status of AIS in sports medicine and exercise
physiology.
1. McMahon et al. (24) evaluated 53 subjects who performed knee extension
stretches 4 times∙wk-1 for 4 wks. The increase in ROM was statistically significant
after the 1st wk of AIS and in static stretches after 2 to 4 wks. The AIS increase
in ROM was significantly greater than for the static stretch exercise.
2. Liemohn et al. (13) studied 30 subjects who performed 9 exercises of straight leg
raise in 3 wks. Both modes of stretching significantly increased ROM, but AIS
increased ROM significantly more than the static stretch exercise.
3. Marino et al. (19) evaluated 30 subjects who were doing the straight leg raise
stretch exercise 3 times∙wk-1 for as long as 13 wks. They reported that only the
AIS significantly increased ROM. As to the static stretch increase in ROM, it was
not significantly different from the control group.
4. Middag and Harmer (25) reported on 30 subjects who performed 5 times∙wk-1 for
3 wks knee extension stretches. AIS increased ROM more than 11% versus the
8% by static stretch, but the difference was not statistically significant.
In 2 of these 4 studies, AIS increased joint ROM significantly more than static stretch. In
the Middag and Harmer`s (25) study, AIS increased more but the difference was not
significant, and in Marino et al. (19) study, only AIS significantly increased ROM. Hence,
the studies point out that AIS attains greater or at least the same increase in joint angles
of the hamstring muscles than static stretch.
In the Lopez-Bedoya et al. (15) study, the findings indicated that static stretch increased
the hamstring ROM more than AIS and more than hold-relax stretching. However, AIS
was not correctly defined in the study, and the study procedures did not follow the ideas
of Mattes book published in 2000, although the book was in the reference list of the
study. Relaxation of the hamstring muscles in AIS exercises is specified incorrectly. The
authors are suggesting that assisted AIS is the same as assisted active static stretches
(AASS) with a 2-sec rest between repetitions and that during this 2-sec rest the muscle
is relaxing. For example, “Training session was thus: 4 x 12 x (AASS 2 sec) with a 2-sec
rest between repetitions and a 50-sec rest between series.” Relaxation of hamstrings is
not taking place in this procedure. Hamstrings are truly relaxed in AAIS (assisted AIS),
66
where the stretching person is actively raising the leg as far as possible, and the
assisting therapist is only finishing the stretch lightly, with less than 4.5 Nm torque.
Since relaxation of the muscle does not happen in AIS exercises in the study, one
essential part of the effect of AIS on ROM is missing and, therefore, the conclusion of
the study is not valid. AIS might as well be increasing ROM more than static stretch, but
the study is not able to give the correct estimate. Same authors, this time in a different
order, Vernetta-Santana et al. (29) published in 2015 another study on AIS. The study
sets out to confirm that AIS will significantly increase joint ROM, but will not weaken
significantly peak isometric force of the hamstring muscles. Definition of AIS is the same
as in the previous Lopez-Bedoyan et al. (15) study with the same incorrect specification
of relaxation of muscles. Therefore, the conclusions of the study are not likely to be
reliable.
DISCUSSION
Active Isolated Stretching has been developed for more than 40 yrs, but its scientific
basis has probably not been demonstrated until the earlier attempts by Mattes to get the
research community to study AIS. But that there are still concerns as explained earlier.
The suggested mechanisms of action of AIS should undergo further studies. After
possible confirmation by research, these mechanisms would be a valuable tool of AIS in
rehabilitation after sport injuries.
In fact, in this regards, Mattes made a 40-yr effort in developing and studying ~120
stretches for his 2012 book on AIS. The number of stretches is large and can serve the
needs of rehabilitation in physiotherapy. The book has instructions both for stretches
made by the client or patient him- or herself and/or by the help of an assisting person.
Mattes would call the self-made stretches “active”, but it is contrary to the research
community terminology. A large number of stretches for muscles and parts of muscles
are needed in rehabilitation. AIS can isolate and focus the stretch more precisely than
static stretches. For example, there are 6 AIS stretches for the hamstring muscles
compared to two stretches in static stretching.
Strength training is also needed in rehabilitation and Mattes published in 2006 a book
on strength training (22). The main idea of the book is similar to AIS in focusing strength
exercises on each muscle if possible. During the 4 decades since the 1970s, several
hundred AIS therapists have applied AIS to sport injuries and musculoskeletal
problems. Rehabilitative AIS exercises are based on physiological principles. AIStherapists
have applied AIS in sports teaching, coaching, and assisted stretching. There
is some indication that in elite level sports, where competition is especially hard and
rewards high, AIS has made a breakthrough and many athletes prefer using it. This may
have increased the use of AIS in sports, although there has been a tendency by
athletes to hide the use of AIS in order to be more competitive. AIS therapists have also
been teaching and training AIS to ordinary people. Mattes would suggest that stretching
is almost a daily requirement, as muscles shorten, stiffen, and/or become tense from
67
work, training, and/or stress. In fact, that is one reason he published a book with the title
“Specific Stretching for Everyone” with instructions for 99 AIS stretches (23).
It is interesting and questionable as well that sports medicine research has shown only
so little interest in AIS. At least on the internet pages of the National Academy of Sports
Medicine (NASM) is a text on “Current Concepts in Flexibility Training”, and AIS is one
alternative stretching method (27). Active Isolated Stretches are suggested for warm-up
before sports competitions or high-intensity exercises. But, NASM defines AIS in a
markedly different way than Mattes. Relaxation of the muscle takes place in NASM`s
definition of AIS, but stretching along the stress line of muscle is missing. When
checking videos of the four example stretches of NASM for biceps femoris, quadriceps,
adductors, and pectoral muscles, it appears that they are not consistent with the AIS –
stretches in Mattes books of 2000 and 2012. Both relaxation of muscle and stretching
along the stress line of muscle are required in AIS, and the definition that NASM is
using for AIS is deficient. Without stretching along the stress line of muscle, stretches
are producing less ROM, and also other positive effects of AIS are missing. This may be
one reason, why the medical research community has lost the willingness to study AIS.
CONCLUSIONS
Aaron L Mattes in his many experiments succeeded in finding that stretching along the
line of stress of the muscle and relaxation of the muscle to be stretched in each
repetition of the stretch would diminish the resistance to stretching. Based on this
finding, it has been demonstrated that AIS stretches are performed with less torque than
static stretches of hamstring and calf muscles. Four studies show that AIS would attain
greater or at least the same increases in joint ranges of hamstring muscles as the static
stretches. The findings should be confirmed by additional scientific research.
ACKNOWLEDGMENTS: Special thanks for valuable suggestions concerning the text
to MD, PhD, Associate Professor Katriina Kukkonen-Harjula, Rehabilitation, South
Karelia Social & Health District, Lappeenranta, Finland
Address for correspondence: Dr. Pertti Kukkonen, Espoo, Finland, Email: kohdeven
@gmail.com
Journal of Exercise Physiologyonline
April 2019
Volume 22 Number 2
Editor-in-Chief
Tommy Boone, PhD, MBA
Review Board
Todd Astorino, PhD
Julien Baker, PhD
Steve Brock, PhD
Lance Dalleck, PhD
Eric Goulet, PhD
Robert Gotshall, PhD
Alexander Hutchison, PhD
M. Knight-Maloney, PhD
Len Kravitz, PhD
James Laskin, PhD
Yit Aun Lim, PhD
Lonnie Lowery, PhD
Derek Marks, PhD
Cristine Mermier, PhD
Robert Robergs, PhD
Chantal Vella, PhD
Dale Wagner, PhD
Frank Wyatt, PhD
Ben Zhou, PhD
Official Research Journal
of the American Society of
Exercise Physiologists
ISSN 1097-9751
Official Research Journal
of the American Society
of Exercise Physiologists
ISSN 1097-9751
JEPonline
REFERENCES
1. Alter MJ. Science of Flexibility. (3rd Edition). Human Kinetics, 2004.
2. Ben M, Harvey LA. Regular stretch does not increase muscle extensibility: A
randomized controlled trial, Scand J Med Sci Sports. 2010;20:136-144.
68
3. Blazevich AJ, Cannavan D, Waugh CM, Miller SC, Thorlund JB, Aagaard P, Kay
AD. Range of motion, neuromechanical, and architectural adaptations to plantar
flexor stretch training in humans. J Appl Physiol. 2014;117:452-462.
4. Chan SP, Hong Y, Robinson PD. Flexibility and passive resistance of the
hamstrings of young adults using two different static stretching protocols. Scand
J Med Sci Sports. 2001;11:81-86.
5. Folpp H, Deall S, Harvey LA, Gwinn T. Can apparent increases in muscle
extensibility with regular stretch be explained by changes in tolerance to stretch?
Aust J Physiother. 2006;52:45-50.
6. Freitas SR, Mendes B, LeSant G, Andrade RJ, Nordez A, Milanovic Z. Can
cronic stretching change the muscle-tendon mechanical properties? A review:
Scand J Med Sci Sports. 2018;28:794-806.
7. Gajdosik RL. Effects of static stretching on the maximal length and resistance to
passive stretch of short hamstring muscles, JOSPT. 1991;14:250-255.
8. Gajdosik RL, Linden DWV, McNair PJ, Williams AK, Riggin TJ. Effects of an
eight-week stretching program on the passive-elastic properties and function of
the calf muscles of older women. Clinical Biomechanics. 2005;20:973-983.
9. Gajdosik RL, Allred JD, Gabbert HL, Sonsteng BA. A stretching program
increases the dynamic passive length and passive resistive properties of the calf
muscle-tendon unit of unconditioned younger women. Eur J Appl Physiol. 2007;
99:449-454.
10. Guissard N, Duchateau JA. Effect of static stretch training on neural and
mechanical properties of the human plantar-flexor muscles. Muscle & Nerve.
2004:248-255.
11. LaRoche DP, Connolly DAJ. Effect of stretching on passive muscle tension and
response to eccentric exercise. Amer J Sports Med. 2006;34:1000-1007.
12. Law RYW, Harvey LA, Nicholas MK, Tonkin L, De Sousa M, Finniss DG. Stretch
exercises increase tolerance to stretch in patients with chronic musculoskeletal
pain: A randomized trial. Physical Therapy. 2009;89:1016-1026.
13. Liemohn W, Mazis N, Zhang S. Effect of active isolated and static stretch training
on active straight leg raise performance. Med Sci Sports Exerc. 1999;31(5):
S116.
14. Longo A. Active isolated stretching: An investigation of the mechanical
mechanisms. Brock University: Ontario, Canada, 2009. Internet, June 2018.
69
15. Lopez-Bedoya J, Vernetta-Santana M, Robles-Fuentes A, Ariza-Vargas L. Effect
of three types of flexibility training on active and passive hip range of motion. J
Sports Med Phys Fitness. 2013;53:304-311.
16. Magnusson SP, Simonsen EB, Aagaad P, Dyhre-Poulsen P, McHugh MP, Kjaer
M. Mechanical and physiological responses to stretching with and without
preisometric contraction in human skeletal muscle. Arch Phys Med Rehabil.
1996;77:373-378.
17. Magnusson SP, Simonsen EB, Aagaard P, Sorensen H, Kjaer M. A mechanism
for altered flexibility in human skeletal muscle. J Physiol. 1996;497(1):291-298.
18. Magnusson SP. Passive properties of human skeletal muscle during stretch
maneuvers: A review. Scand J Med Sci Sports. 1998;8:65-77.
19. Marino J, Ramsey JM, Otto RM, Wygand JW. The effects of active isolated vs.
static stretching on flexibility. Med Sci Sports Exerc. 2001;33(5):supplement 1:
S10.
20. Mattes AL. Aaron Mattes` Active Isolated Stretching. Sarasota, Florida, 2000.
21. Mattes AL. Aaron Mattes` Active Isolated Stretching. Sarasota, Florida, 2012.
22. Mattes AL. Active Isolated Strengthening: The Mattes Method. Sarasota,
Florida, 2006.
23. Mattes AL. Specific Stretching for Everyone. Sarasota, Florida, 2000.
24. McMahon T, Catlin P, Cooper A, Fleckenstein D, Maloney P, Marxe R. Effect of
active isolated versus static stretching in asymptomatic adults. J Orthop Phys
Ther. 1997;25(1):Combined Sections Meeting, PO51.
25. Middag TR, Harmer P. Active-isolated stretching is not more effective than static
stretching for increasing hamstring ROM. Med Sci Sports Exerc. 2002;34(5):
Supplement 1, S151.
26. Myers TW. Anatomy Trains, Myofascial Meridians for Manual and Movement
Therapists. (2nd Edition). Elsevier, 2008.
27. National Academy of Sports Medicine (NASM). Current Concepts in Flexibility
Training. (Internet) February 5, 2019.
28. Reid DA, McNair PJ. Passive force, angle, and stiffness changes after stretching
of hamstring muscles. Med Sci Sports Exerc. 2004;36:1944-1948.
70
29. Vernetta-Santana M, Ariza-Vargas L, Robles-Fuentes A, Lopez-Bedoya J. Acute
effect of active isolated stretching technique on range of motion and peak
isometric force. J Sports Med Phys Fitness. 2015;55:1299-1309.
30. Waye D, Mielke A. Active isolated stretching for runners. Peak Running
Performance. May/June, 2010.
31. Weppler CH, Magnusson SP. Increasing muscle extensibility: A matter of
increasing length or modifying sensation? Physical Therapy. 2010;90(3):438-
449.
32. Ylinen J, Kankainen T, Kautiainen H, Rezasoltani A, Kuukkanen T, Häkkinen A.
Effect of stretching on hamstring muscle compliance, J Rehabil Med. 2009;41:
80-84.
Disclaimer
The opinions expressed in JEPonline are those of the authors and are not attributable
to JEPonline, the editorial staff or the ASEP organization.
Myofascial triggers points: What are they ?
by: Hans de Wit
Did you know that the Skeletal muscle structure (also called voluntary muscles) is the largest single organ of the human body and can weight 40% and more of our total body weight ? All this muscle mass can be divided into an astounding number of 696 individual muscles, that are made up by millions of fibres , nerves and blood vessels.
Today I hope to shed some light on why this complex network of soft tissues is playing a much larger role in your health than you might think. And also why its is so often overlooked by medical specialists who prefer looking at bones, joints , bursae and nerves for diagnosis and treatment.
Our muscles are extremely subject to the winding and grinding of our daily activities and even more so to our daily lack of activities. This causes trigger points in the fibers that can be classified into Active trigger points and latent trigger points.
They form as a local contraction in a small number of muscle fibers in a larger muscle or muscle bundle. The integrated hypothesis theory states that trigger points form from excessive release of acetylcholine which produces sustained depolarization of muscle fibers.
Unrecognized myofascial headaches, shoulder pain and low back pain that have become chronic are a major cause of lost time in the workplace and absenteeism in employees. Research has pointed out that chronic pain costs the american economy billions of dollars each year, and South Africa will be no different.
Some of the main causes of trigger points and pain are acute overload of muscles, overworking of muscles, chilling of the muscle fibers and traumatic events. Often times different diseases can cause soft tissue pain as well, with the heart, gallbladder and other visceral diseases being the major contributors. Emotional stress however , can play an even greater roll, causing the highest number of patients with muscle pain.
Trigger point are renowned for their ability to generate referred pain throughout your body. You might have a devastating headache on your temporal region of your skull , however the cause of your headache will be found down in your neck. This phenomenon can become very complex with different layers of muscle pain and stiffness surrounding a specific joint or vertebral body.
This is why different phases of rehabilitation is necessary. Stretch therapy will slowly remove all muscle stiffness and lack of range of motion. With this the outer and inner layers can be gently entered and trigger point therapy can be applied, putting pressure on very precise points in your body.
The therapist can also apply a stretch and spray technique. This technique involves an agent called vapocoolant, research has indicated that the use of a active coolant on the skin in combination with a stretch can inactivate trigger points very effectively.
After being diagnosed with right knee medial tibial plateau insufficiency fracture with a background of osteoarthritis medial meniscus and posterior root tear and varicose veins, I've been attending StretchingSA Pretoria East every week and have found such a difference even after a few sessions - pain has now gone and I can only say it is amazing the amount of increased motion I now have!
My knees were swollen and in pain after 'Om Die Dam Ultra 50km'. I've tried Crossfit, physiotherapy and biokinetics, and although it helped, I just couldn't get rid of the pain. Thanks to AIS stretch therapy and in particular trigger point release done by Monica from StretchingSA Roodepoort, I've been able not just to finish the Comrades 2023, but also improved my PB by 30min with hardly any serious pain or niggles!
I worked closely with a physiotherapist and later, a biokineticist and performed all exercises given to me daily. I got stronger but still struggled with pain, flexibility and movement which meant that my hips and back took strain to accommodate my unnatural way of walking. I met with Ryno at StretchingSA and after a couple of months, I regained the full range of movement in my ankle and calf muscle.
Lenka was incredible at relieving the discomfort in my feet in our session. It got me up and running again super quickly and has kept the condition under control since. I would highly recommend Lenka for any ankle/foot-related issues especially if you’re looking for someone to not just treat symptoms but underlying causes.
Ever since my weekly stretch routine, I have been much more flexible and not so stiff after music gigs, golf, tennis, squash and paddle tennis. I would recommend Carla Swart from StretchingSA Pretoria East!
Having tried various therapies without success, I discovered StretchingSA and Ryno van den Berg. His methods were patiently delivered, methodical, and scientific – and they have worked. I am back to running.
With persistent treatment, we went from barely being able to open the hip due to intense pain and tightness to being able to open fully with barely any discomfort.
We started with stretching and soon I could feel a difference. When I began the treatment, I could not reach my toes bending forward. After each treatment, I could bend a little further. Today I can confidently say that I can touch my toes even before having warmed up a bit.
Carla was professional and friendly and after a brief session with her, I was hooked. I started going to regular weekly sessions and can report that my lower back pain is gone.
Attending the stretch classes on a regular basis has been one of the best things I could have done for my body and I wholeheartedly recommend it to anyone who needs to improve their posture and take care of hardworking muscles.
I am now approaching my 10th session with Carla and every week I could experience the increased range but also the depth of the stretch, reaching deeper lying muscles that would otherwise never get activated. I just love the extra range, mobility, and flexibility I gained.
I am thankful to Ryno for his professional help and sensitive way of helping patients. I am convinced that we have achieved the objective of at least deferring further possible surgical interventions.
For the first time in a long while, I started to believe that my injury could be treated without getting an invasive procedure. Thank you Ryno from StretchingSA Pretoria East not just for the treatments but also for your positive input into my life!
I am sold on STRETCHINGSA...I will never go back to a chiro or physio for such issues...I highly recommend them! Thank you Gary at StretchingSA Centurion!
I suffer from jaw clenching and often struggle with general stiffness. Lenka has been amazing in helping relieve tightness and making exercising easier! I cannot recommend her enough. Knowledgeable, professional, and kind.
Deidre Schoeman
There was no reason to feel nervous about going to Lenka for a stretching session. Lenka has the ability to listen to your body. Therefore, she will never push the body against its will but also knows when to push harder so the muscles can relax and the body can heal.
Absolutely amazing session. Lenka is incredibly kind, patient, and professional. I saw her after moving house when my back, neck and shoulders were in complete agony, and she sorted me out in just one session. It was the best money I have ever spent.
Dex Kelly
I sustained a shoulder injury after a fall. In the 1st session, StretchingSA (Lenka Van Wyngaardt) identified the precise nature of the injury. After 4 weekly sessions, I regained full use of my shoulder.
I was introduced to Lenka, she has been stretching all my muscles and joints for the past couple of months now, I have my swing back, I can get up and down easier and I can work all day in my garden.
It only took 5 sessions to achieve this result, with minimal effort on my part with exercises at home. I now go for a once-monthly “maintenance” stretch (this is my choosing) as we do a whole body stretch and I feel 15 years younger when I leave!
Competent, knowledgeable, diligent, firm and yet gentle. Everyone who requires rehabilitative therapy deserves to have one such as she! Lenka you have made a world of difference to my damaged body, and soul. I’m very grateful to have found you.
After only a few sessions, I noticed an improvement that continued weekly. About 4 months down the line I sometimes must stop and think which hand was painful as I no longer experience any discomfort.
I went to Ryno at StretchingSA Pretoria East Moreleta Park. It was by far the only treatment that made a difference. Although the treatments were not without discomfort, the relief afterwards and the progress that was made was worth it.
I'm extremely grateful to Ryno, not only for his services but also for his motivational words and encouragement during each treatment. I'm convinced that I am stronger than ever thanks to his help.
After trying out many other options to address a potential neurological issue causing pain in my left foot, I discovered stretch therapy from StretchingSA. We’re not 100% there yet, but I have found much relief and can enjoy long walks in nature again!
Within a few weeks, I have seen and experienced the most amazing changes through regular stretch therapy. I would gladly recommend stretch therapy for everyone as it is natural and definitely aids in the recovery and daily functioning of one’s body.
One of my friends recommended I see Hayley from StretchingSA George. After just two sessions with Hayley, my pain was gone and I managed to run my long distances again pain-free.
I encourage you to read up on the benefits of StretchingSA’s stretching techniques and how they can benefit you. I am into my 7th treatment session and WOW what a difference in my symptoms and overall muscle condition.
I have been seeing Hayley for 2 months now and can feel the progress that I have made over this time. I have found that the AIS Stretching has helped me gain strength in my lower back and the constant discomfort and aching has eased tremendously.
Monica and stretch therapy changed my life! I can feel that every session makes a difference. Monica is an amazingly kind and friendly stretch therapist who has never pushed me beyond my pain levels. I can only thank Monica for how much the quality of my life has improved.
I saw Ryno from StretchingSA Pretoria-East (Moreletapark) for a 30-minute session and by stretching out the correct muscle fibers, I immediately experienced relief. I can happily confirm, that my leg has recovered completely.
I started with Ryno and at first, I must say I thought it was an unsuccessful solution. But I stayed and gave it time. The results were up and down but it did not seem to work as I was still in pain. Now for 2 weeks, I am without pain and this is all due to Ryno's hard work and treatments!
I started seeing Ryno a few months ago and my life has only improved since. Not only can you see the difference in your training, but in your day to day life as well. Being more flexible allows you to be more effective in every aspect of your life.
StretchingSA is an absolute must for any sports, mobility, or even old unattended injuries. If you are committed to dedicating time for recovery, you will heal! I know I speak from someone who thought they would have to live with pain for the rest of their life. It does change, it just needs hard work.
Then I found Stretching SA, this treatment started to work after only a few treatments. I started to experience permanent mobility in my knees again. After only 3 months of two sessions a week, I could walk normally and are pain-free.
After 3 months of treatment, I can testify that my lower back pain has been treated successfully. From now on, I will visit Ryno once a month or even every second month in order to maintain the flexibility of my muscles. I am truly grateful for Ryno and StretchingSA.
I have been seeing Hayley for the past 2 months now every week. I can feel and see a huge improvement in my training at the gym and in my running. I feel lighter on my feet and the stretching has made my running a lot easier. It has also helped keep me injury-free.
Since I’ve been seeing Hayley on a weekly basis, I’ve broken 12 South African records across 2 bodyweight categories and it all boils down to one simple difference...the strengthening work, treatment or injuries and postural alignments she has done over the last couple of months.
I was so impressed that I brought my daughter along; she was struggling with a serious knee injury. Hayley’s assessment was spot on, her treatment even better. With every session, the stretching becomes easier, so much so that I am actually looking forward to my next session
From my first session with Hayley I could feel a difference in my body. Less stiffness and less pain. My body feels lighter after a stretch session with her. She also makes a lot of effort to get to the core of the problem and is always friendly, caring and willing to help. I am always looking forward to my next stretching session!
Deon Fourie
Within the 1st week, I knew I was in the right place! I would recommend stretching therapy to anyone and especially to athletes who are serious about their sport! Keep it injury-free, get yourself a stretch therapist! Get Haley she's really one of the best I've worked with.
Within completing the 5 sessions I have seen major improvements; my leg mobility has strengthened to the point of forgetting I even had surgery. I have made a full recovery and slowly back to where I was. Thanks to Louretha for all the sessions which have changed my life.
After 6 months my lower back improved with 80%. Stretch Therapy changed my life. 18 years of pain started improving within months. I can’t wait to feel the end result. I would recommend Stretch Therapy for anyone with chronic pain and structural problems!
I came to see Hayley for a full-body stretch and never felt better. I am not very flexible, but Hayley managed to get me into unheard-of positions, which helped heaps. Hayley is a great therapist and will take good care of anyone no matter the problem, wherever she practices.
Within 3 months of treatment, the results were remarkable! Since then I have consulted Ryno for various other treatments for my hip and lower back and I'm astounded by the remarkable improvement after each session. Truly a Stretch Therapist I can recommend!
Flexibility is not only necessary for a better range of motion and movement, but a hidden jewel to any rehabilitation, prevention and cure program. Active Isolated Stretching, Strengthening and Balancing is definitely the way of the future from the injured patient to the sports person.
Then I discovered Ryno van den Berg at Stretching SA. After 4 sessions I could feel and see a difference in my throwing technique and my hamstrings are a lot more flexible. I can touch my toes now, which was something I could never do before.
The first session already resulted in major pain relief and by week four, I had my old self back. It’s great to know that should I ever experience something similar, StretchingSA will be there to assist. I can strongly recommend Ryno and StretchingSA.
After 3 months of treatment, I can testify that my lower back pain has been treated successfully – I only have some pain when I’ve had a tough day standing for long hours but other than that I know I have found the correct treatment. I am truly grateful for Ryno and StretchingSA.
From my own experience, I can, with great confidence, recommend Ryno as a very professional and helpful therapist, as well as the stretching technique, that focuses on stretching the surrounding muscles and ligaments in order to improve mobility and decrease pain.
After 5 sessions I no longer had the numbing pressure of lower back pain, after 10 sessions my lower back pain had almost completely disappeared, and after 15 sessions where we are now, I am able to do an acrobatic trick involving my back.
I would strongly recommend Stretch Therapy to anybody struggling with not only stiffness but inadequate mobility of the joints and pain. The Stretch Therapy didn’t only help me regain my suppleness, but also strength and confidence to move and get my arm back into top form. Thank you, Ryno!
When we called for appointments he didn’t hesitate to come over to our house and started treatments right away. I was blown away by his professionalism and friendly approach to his patients and truly can recommend him as a practitioner that will spend a lot of time and effort on each and every patient he will ever see.
I picked up an Injury when I was 21 years old, on the Rugby field, in my left leg. For 15 years I struggled with spasms and pain in all areas of my left leg from the upper thigh to the calves. Thousands of hours with different medical methods and options were perused with no improvement at all.
I believe stretch therapy should be incorporated into everyone’s lives as I have never felt so supple and flexible as to when I started practicing with Louretha. Stretch therapy has helped to increase my suppleness, it has definitely improved my extension with all joints; so I can concentrate more on my golfing and better improve my swing.
Beste Louretha, hiermee net ‘n klein gebaar om dankie te se vir jou ondersteuning, hulp en aanmoediging deurentyd met my behandeling! Ek het begin by jou met ongelooflike erge pyn, maar ek voel deesdae soos ‘n nuwe mens!
Louretha Jacobs did an evaluation and said she could help me with stretch therapy. Louretha was always very professional and friendly and she continuously encouraged me. Although progress was slow and the sessions were sometimes painful I could see progress after about four weeks. I would highly recommend stretch therapy.
We, Annika and Bianca Strydom are Biathle athletes (swimming and running). We came first and second for consecutive years. We have attended physiotherapy and stretching sessions with Louretha for injuries for a few years. She is very knowledgeable about her profession and very helpful with information around the injuries...
I would like to take this opportunity to share with you how StretchingSA (AIS) has been beneficial to me and how much it has helped my life and injuries. I used to be a rugby player and went on with normal conditioning on the field and at a gym. I have been struggling with nerve pain down my arm since I can remember.
Ek kan nie genoeg beskryf hoe strek terapie Aidan so vinnig laat herstel het nie. Louretha Jacobs was uiters professioneel en deeglik, sy het ook vir Aidan rehab huiswerk gegee om sy maagspiere te versterk wat self ‘n groot verskil gemaak het aan die herstel van sy rugspiere.
This is when I discovered StretchingSA and I contacted Ryno van den Berg. I have been going to StretchingSA now for 2 treatments per week for about 3 months and WOW! Last month was the first time in the last 14 years that I were without any pain for 3 consecutive days and then I had a whole week without any pain!
I have yet to reach the optimum level of a pain-free life but we are well on our way in achieving this, however, I cannot translate in words, the relief of pain and spasms I have experienced since starting treatment with Ryno at StretchingSA. I can only thank Ryno for the effort and work he has done and continues to do for me.
I cannot thank Ryno enough for the past few weeks and the sessions I had with him. After each session, I was amazed by his knowledge about the body and the effects his treatment had on my body. The pain was gone after three sessions with him and the pins and needles have faded.
If you surround yourself with the right people, anything is possible... Surround yourself with only people who are going to lift you higher... People who are going, to be honest with you and look out for your best interest, thanks StretchingSA for being part of my team!
StretchingSA helped me through an intensive Stretch Therapy rehabilitation program. My Joint range of motion, stability, flexibility, strength, and balance improved drastically. I’m so fortunate to have the cause of my problem been taken care of with no pain anymore.
As a Stretch Therapist, Ryno is treating my injured knee. My joint range of motion, flexibility, strength, and balance improved drastically. I sleep without pain. Getting in and out of a car is not an effort anymore. It is possible to use stairs in a normal way without pain. I started doing needlework again. I am so fortunate to be treated by Ryno.
I want to stretch how impressive this unique form of rehabilitation is for me, seeing that I have tried so many different forms of treatment and nothing ever had the wonderful results that I am experiencing right now. Any athlete with frequent spasms or injury that gives them trouble should go to no other place. Book your sessions now!
When I walked out of my first session with Hans it literally felt like I had been given a new pair of legs and a new back, my first session felt like a miracle cure. I see Hans on a weekly basis and it’s the only thing that keeps me going. StretchingSA has improved my quality of life; I am completely pain-free and have been pain-free for 3 full months.
I’ve been struggling with my shoulder (rotator cuff) since October 2014. I’ve experienced a lot of pain and discomfort especially when I sleep at night. I went for two sessions with Ryno van den Berg the Stretch Therapist. The pain and discomfort stopped completely. My rotator cuff is completely healed.
After having a full knee replacement at the age of 63 I was left with one new very sore and extremely stiff knee and one old, painful and stiff knee. The doctors were not happy with my recovery but soon after I was referred to Ryno and StretchingSA, my life changed. Today I can enjoy my new knee and the days of being in constant pain...
I went to StretchingSA and since I have been there my si-joint has recovered and improved and I can bowl again without any discomfort. I can definitely recommend Stretching SA for anyone moving with discomfort and struggling with their mobility. I got more out of Stretching SA than I hoped for. A big thanks to Ryno and Stretching SA!
Stretching SA helped me recover from an injury I had for decades and the methods and maneuvers been used was focused on my problem area and not a generic one solution for all approach. Thank you, Ryno, for helping me back on my knees again. I will recommend this approach to improve, recover or support all levels of athletes...
One morning two months ago I woke up with severe pain again, decided to make an appointment with Ryno the stretch therapist, and the decision was made to go for stretch therapy. After 12 rehabilitation sessions, I was pain-free…I could walk for longer distances, sit for longer periods of time at the office...
I prefer working with my man Hans at StretchingSA, making sure I'm stronger and faster than ever… especially good in getting some work done with stretch therapy before my big games. Thank you guys for always helping me being the best I can be.
Hans de Wit has been working with the Bulls and Blue Bulls players for the past two years. Hans is a stretch therapist and he has made a big difference in our system with regards to recovery and prevention of injuries. Hans definitely had a big hand in all the success we had the past few years.
It is with great pleasure that I recommend Hans de Wit. Hans is an excellent Stretching Therapist and consists of all the skills needed to treat his patients successfully. If you have any further questions, please feel free to contact me.
I have had the pleasure of working with Hans de Wit whilst on assignments abroad, treating top VIP clients and patients. Although a true expert in his field, Hans is gracious and shares his knowledge and skills generously. He exhibits outstanding skill and knowledge and exudes a passion for improving the lives of others.

 There are as much as 72 muscles surrounding your hips and upper leg. not even to mention the hordes of muscle structures that builds up from the hips into your back. When it comes to bones, the socket is made of three joined pelvic bones – the ilium, the ischium and the pubis. The hip joint is made up of four bones.
There are as much as 72 muscles surrounding your hips and upper leg. not even to mention the hordes of muscle structures that builds up from the hips into your back. When it comes to bones, the socket is made of three joined pelvic bones – the ilium, the ischium and the pubis. The hip joint is made up of four bones.


