 A study done in Canada, once again showed us that holding your stretches for long periods (45 seconds) is not good for your athletic performance, and even impair your warm up. If you like to exercise, please don’t warm up with long stretches.
A study done in Canada, once again showed us that holding your stretches for long periods (45 seconds) is not good for your athletic performance, and even impair your warm up. If you like to exercise, please don’t warm up with long stretches.
The purpose of the study was to investigate the effect of an acute bout of lower limb static stretching on balance, proprioception, reaction, and movement time.
The conclusion was that an acute bout of static stretching impaired the warm-up effect achieved under control conditions with balance and reaction/movement time.
Methods: Sixteen subjects were tested before and after both a static stretching of the quadriceps, hamstrings, and plantar flexors or a similar duration
control condition. The stretching protocol involved a 5-min cycle warm-up followed by three stretches to the point of discomfort of 45 seconds each with 15-s rest periods for each muscle group. Measurements included maximal voluntary isometric contraction (MVC) force of the leg extensors, static balance using a computerized wobble board, reaction and movement time of the dominant lower limb, and the ability to match 30% and 50% MVC forces with and without visual feedback.
Results: There were no significant differences in the decrease in MVC between the stretch and control conditions or in the ability to match submaximal forces. However, there was a significant (P 0.009) decrease in balance scores with the stretch (2 9.2%) compared with the control (1 17.3%) condition. Similarly, decreases in reaction (5.8%) and movement (5.7%) time with the control condition differed significantly (P 0.01) from the stretch-induced increases of 4.0% and 1.9%, respectively.
Conclusion: In conclusion, it appears that an acute bout of static stretching impaired the warm-up effect achieved under control conditions with balance and reaction/movement time.
Effect of Acute Static Stretching on Force,
Balance, Reaction Time, and Movement Time
DAVID G. BEHM, ANDREW BAMBURY, FARRELL CAHILL, and KEVIN POWER
School of Human Kinetics and Recreation, Memorial University of Newfoundland, St. John’s, Newfoundland, CANADA
ABSTRACT
BEHM, D. G., A. BAMBURY, F. CAHILL, and K. POWER. Effect of Acute Static Stretching on Force, Balance, Reaction Time, and
Movement Time. Med. Sci. Sports Exerc., Vol. 36, No. 8, pp. 1397–1402, 2004. Purpose: The purpose of the study was to investigate
the effect of an acute bout of lower limb static stretching on balance, proprioception, reaction, and movement time. Methods: Sixteen
subjects were tested before and after both a static stretching of the quadriceps, hamstrings, and plantar flexors or a similar duration
control condition. The stretching protocol involved a 5-min cycle warm-up followed by three stretches to the point of discomfort of
45 s each with 15-s rest periods for each muscle group. Measurements included maximal voluntary isometric contraction (MVC) force
of the leg extensors, static balance using a computerized wobble board, reaction and movement time of the dominant lower limb, and
the ability to match 30% and 50% MVC forces with and without visual feedback. Results: There were no significant differences in
the decrease in MVC between the stretch and control conditions or in the ability to match submaximal forces. However, there was a
significant (P � 0.009) decrease in balance scores with the stretch (2 9.2%) compared with the control (1 17.3%) condition.
Similarly, decreases in reaction (5.8%) and movement (5.7%) time with the control condition differed significantly (P � 0.01) from
the stretch-induced increases of 4.0% and 1.9%, respectively. Conclusion: In conclusion, it appears that an acute bout of stretching
impaired the warm-up effect achieved under control conditions with balance and reaction/movement time. Key Words: STABILITY,
ISOMETRIC FORCE, PROPRIOCEPTION, FLEXIBILITY
Stretching is commonly utilized to increase the range
of motion (ROM) around the joint (12,19) and theorized
to improve athletic performance (28). With the
exception of an increased ROM, recent studies have not
found substantial evidence to support the use of stretching
for improved performance. A number of studies report that
acute and prolonged stretching may actually reduce human
performance through decreases in force (4,14,15) and power
(11,40).
The stretch-induced decreases in force and power have
been attributed to impairments in neural output (2,4,13) as
well as changes to the musculo-tendinous unit (MTU)
(13,34). Fowles et al. (13) demonstrated an increase in
fascicle length of the soleus and lateral gastrocnemius of a
single subject with 30 min of stretching. Studies have reported
both decreases (24,35) and no change (23) in MTU
passive resistance or stiffness with stretching. MTU stiffness
incorporates the muscle, tendon, and other associated
connective tissue and can determine the effectiveness and
rapidity by which internal forces generated by the muscle
are transmitted to the skeletal system (38). Among the
functions of the intrafusal (includes stretch receptors) muscle
fibers, Golgi tendon organs and other proprioceptors is
to aid in the maintenance of balance (26) and detection of
the position of the body in space (proprioception) (8,10).
Acute changes in MTU length, stiffness, force output, and
muscle activation could alter the ability to detect (afferent
proprioception) and respond (efferent muscle activation) to
changes in the immediate environment. Stretch-induced impairments
might affect overall balance and stability or limb
proprioception. Furthermore, a more compliant MTU
(greater muscle and connective tissue slack) in conjunction
with a disturbed activation of the muscle could alter reaction
(RT) and movement (MT) times. There have been no studies
reporting on the effects of an acute bout of stretching on
balance, proprioception or reaction/movement time.
Balance involves the interaction of automatic postural
and voluntary motor commands of both the trunk and limb
musculature (6,30). Automatic postural responses are modulated
by both trunk and leg inputs (5), with the central
nervous system (CNS) performing anticipatory postural adjustments
when expecting self-inflicted postural perturbations
(1). Because under conditions of high instability the
CNS may suppress anticipatory postural adjustments, voluntary
responses of trunk and limb muscles to postural
challenges would play a prominent role. Stretch-induced
changes to either the afferent limb muscle responses (proprioception)
or the mechanical output would be expected to
affect the ability to adapt effectively to stability challenges.
At the elite sport level, where milliseconds can mean the
difference between winning and losing, even small changes
in RT, MT, and balance can have a dramatic impact. For
example, differences between the personal best times of the
Address for correspondence: David Behm, Ph.D., School of Human Kinetics
and Recreation, Memorial University of Newfoundland, St. John’s,
Newfoundland, Canada, A1C 5S7; E-mail: dbehm@mun.ca.
Submitted for publication December 2003.
Accepted for publication April 2004.
0195-9131/04/3608-1397
MEDICINE & SCIENCE IN SPORTS & EXERCISE®
Copyright © 2004 by the American College of Sports Medicine
DOI: 10.1249/01.MSS.0000135788.23012.5F
1397
top sprinters in the world can differ by approximately 1%
(i.e., Greene: 9.79 s, Bailey 9.84 s, Christie: 9.87 s, Cason
9.92 s). Thus, even minor changes in RT, MT, and balance
could have important implications for athletic endeavors.
The possibility of stretch-induced impairments to balance,
RT, and MT not only affects sport applications but the loss
of dynamic balance is also a risk factor for osteoporotic
fractures (27). The contributions of RT and MT to dynamic
balance could have implications not only for athletes and
fitness enthusiasts but also for rehabilitation professionals
who prescribe stretching.
The objective of the present study was to examine alterations
in static balance, proprioception, RT and MT, and
force. It was hypothesized based on previous studies that
demonstrated decreases in force and activation as well as
changes in MTU stiffness that all the dependent variables
would be adversely affected by an acute bout of static
stretching.
METHODOLOGY
Approach to the problem and experimental design.
Because a number of the previous studies investigating
stretch-induced force and power decrements used prolonged
stretching routines (15–30 min) of single muscle
groups (4,13) that were not representative of typical stretching
routines, the present study used a moderate volume of
stretching with three lower-limb muscle groups. Subjects
were tested before and after both an acute bout of static
stretching of the quadriceps, hamstrings, and plantar flexors
or a similar duration control condition. The stretching protocol
involved a 5-min cycle warm-up followed by three
stretches to the point of discomfort of 45 s each with 15-s
rest periods for each muscle group (independent variable).
Measurements were conducted over a 20-min period that
included maximal voluntary isometric contraction (MVC)
force of the leg extensors, static balance using a computerized
wobble board, reaction and movement time of the
dominant lower limb, and the ability to match 30% and 50%
MVC forces with and without visual feedback (dependent
variables).
Subjects. Sixteen healthy male university students (age
� 24.1 � 7.4 yr, weight � 71.5 � 15.4 kg, height � 172.3
� 6.5 cm) volunteered for the experiment. All participants
were verbally informed of the protocol, and read and signed
a consent form. Each participant also read and signed a
Physical Activity Participation Questionnaire (PAR-Q: Canadian
Society for Exercise Physiology) to ensure that their
health status was adequate for participation in the study. The
study was sanctioned by the Memorial University of Newfoundland
Human Investigations Committee.
Intervention. Before stretching of both legs, subjects
performed a warm-up procedure consisting of a 5-min cycle
on a cycle ergometer (Monark Ergomedic 828E) at 70 rpm
with 1-kp resistance. The order of quadriceps, hamstrings,
and plantar flexors stretching was randomized. Stretches
were held to the threshold of discomfort for a duration of
45 s with 15-s recovery periods between stretches. Each
type of stretch was repeated three times. Stretching of both
legs included a series of unilateral kneeling knee flexion
(quadriceps), hip flexion with extended leg while supine
(hamstrings), extended leg dorsiflexion while standing
(stretch of the plantar flexors with gastrocnemius emphasis),
and flexed knee dorsiflexion while standing (stretch of the
plantar flexors with soleus emphasis). Stretching was passive
for the quadriceps and hamstrings with the same researcher
controlling the change in the range of motion and
resistance for all subjects. The researcher would extend the
limb to the limits of the participant’s range of motion
without incurring injury. Subjects provided their own resistance
for the plantar flexors stretches with the instructions to
stretch the muscles to the point of discomfort.
For the control condition, subjects performed the 5-min
cycle warm-up and were allowed to rest for approximately
26 min between the pre- and posttesting periods. The 26-
min rest period provided similar pre- to posttest durations
for the stretching and control conditions. The order of control
and experimental stretch conditions was randomized.
Testing. An orientation session involving multiple attempts
(minimum three attempts) for all measures was organized
for all subjects 3–5 d before testing. The order of
testing was randomized. The stretching intervention commenced
2 min after the pretesting session. Postintervention
testing began within 1 min after the stretching routine. The
duration of pre- and posttesting was approximately 20 min
each.
For leg extension MVC force, subjects sat on a bench
with hips and knees flexed at 90°, and the upper leg and hips
restrained by two straps. The ankle was inserted into a
padded strap attached by a high-tension wire to a Wheatstone
bridge configuration strain gauge (Omega Engineering
Inc., LCCA 250). Prestretching, subjects performed two
leg extension MVC. If there was more than a 5% difference
in maximum force output, another MVC was performed.
Only two contractions were permitted poststretching to reduce
the chance of fatigue. Three-minute rest periods were
allocated between contractions. The day-to-day reliability of
the strength test using an intraclass correlation coefficient
(ICC) was determined to be 0.9, with a between test (single
session) reliability of 0.93.
All torques were detected by the strain gauge, amplified
(Biopac Systems Inc., DA 100, and analog to digital converter
MP100WSW) and monitored on computer (Sona
Phoenix PC). All data were stored on a computer at a
sampling rate of 2000 Hz. Data were recorded and analyzed
with a commercially designed software program (Acq-
Knowledge III, Biopac Systems Inc.).
The matching force task used the same set-up as the MVC
test. Once the MVC force was established, grid lines were
provided on the computer, which outlined 30% and 50% of
the MVC force. Subjects were asked to exert sufficient
isometric leg extension force over a 5-s period to match the
gridlines. Visual feedback was always given for the first
three trials of a particular relative force (30% or 50% MVC),
while the computer screen was obstructed from view for the
subsequent three trials. Two-minute rest periods were per-
1398 Official Journal of the American College of Sports Medicine http://www.acsm-msse.org
mitted between attempts. The order of the relative force
matching tasks was randomized. The day-to-day reliability
of the matching force test using an ICC was determined
to be 0.8, with a between test (single session) reliability
of 0.88.
A balance ratio (contact with floor to no contact time) was
calculated by a software program (Innervations, Muncie,
IN) from a 30-s wobble board test (Kinematic Measurement
Systems, Muncie, IN). A metal plate connected to the computer
hardware was placed under the wobble board. When
the perimeter of the wobble board made contact with the
metal plate, the duration and frequency (during the 30-s test)
of contact was recorded by the software. Subjects received
an orientation session for the balance board on a separate
day as well as one to two practice attempts on the day of
testing. The day-to-day reliability of the balance test using
an ICC was determined to be 0.81, with a between test
(single session) reliability of 0.86.
RT and MT were measured by an apparatus developed by
the Memorial University of Newfoundland Technical Services
(Electronics, Newfoundland, Canada). The testing apparatus
consisted of a stop clock (58007, Lafayette Instrument
Company, Lafayette, IN), an analog timer (L15–365/
099, Triton Electronics, UK), a stop clock latch (58027,
Lafayette Instrument Company) that connected the stop
clock and the analog timer, a custom-designed box (62 cm
(length) � 15.5 cm (width) � 9 cm (height)) with the
distance of 50 cm from center of start button to the center of
the stop button, and a trigger plate for the start of the task.
With the device situated on the floor, the task entailed
movement of the dominant foot in response to the illumination
of an incandescent light bulb. The subject would start
with the nondominant foot on the floor and the dominant
foot (ball of foot) placed on the start button. Upon illumination
of the light signal, the subject would release the start
button and move their foot forward to touch the stop button
(50 cm). RT was measured as the time between the illumination
of light stimulus and release of the start button. MT
was measured as the time between the initiation of movement
and the depressing of the stop button. The actions
involved hip flexion, knee extension and plantar flexion. In
order to move as quickly as possible, the quadriceps and
plantar flexors would initiate the movement, while the hamstrings
would aid with the deceleration of the leg to accurately
touch the stop button. Three trials of RT and MT were
performed with 30-s rest periods. The day-to-day reliability
of the RT and MT tests using an ICC was determined to be
0.60 and 0.89 respectively with no significant (P � 0.05)
difference between values for test versus retest. Between
test (single session) ICC reliability measures of 0.79 and
0.93 were recorded for RT and MT, respectively.
Statistical analysis. Data were analyzed using a twoway
ANOVA repeated measures design. The factors included
condition (stretching vs control) and testing (pre- and
postcondition). An alpha level of P � 0.05 was considered
statistically significant. If significant differences (P � 0.05)
were detected, a Bonferroni-Dunn’s procedure was used to
identify the significant change. The means and SEM are
illustrated in Table 1. Reliability was assessed using an
alpha (Cronbach) model ICC (25) with all 16 subjects.
Repeated tests were conducted within 48–72 h.
RESULTS
Overall, significant differences from the control condition
due to the stretching protocol occurred with measures of
static balance, RT and MT.
Force. There was no significant difference between
stretching and control conditions in force output. The stretch
and control conditions experienced similar 6.9% and 5.6%
force decrements, respectively, from the pretest to the
posttest.
Perceived force. Whether visual feedback was or was
not provided, there were no significant differences in the
ability to match 30% and 50% MVC between control and
stretch conditions during the pretest or posttests. The control
condition demonstrated a nonsignificant 18.8% and 10.7%
greater accuracy for maintaining 30% and 50% MVC
posttest.
Balance. Balance scores moved in opposing directions
resulting in a significant change (P � 0.009) for the pre- to
posttest differences between control and stretch conditions
(effect size � 0.11: small). In comparison with the precontrol
sessions, the control condition demonstrated a significant
(P � 0.05) 17.3% improvement in balance scores
postcontrol, whereas the stretch condition showed a nonsignificant
2.2% decrease in balance scores poststretching routine
(Table 1).
Reaction and movement time. Similar to balance
scores, reverse trends for the stretch and control conditions
resulted in significant change for the pre- to posttest differences
with both reaction (P � 0.01, effect size � 1.11:
TABLE 1. Balance, reaction and movement time data (means � SEM).
Pretest Control
Condition
Posttest Control
Condition
Pre- to Posttest
Difference
Pretest Stretch
Condition
Posttest Stretch
Condition
Pre- to Posttest
Difference
Wobble board contacts 10.8 8.9 1.9 8.8 9.0 0.2
(�2.0) (�1.5) 917.3%* (�1.7) (�1.8) 82.2%
Reaction time (RT) 294 ms 277 ms 17 ms 283 ms 294 ms 11 ms
(�27.5) (�10.7) 95.8% (�16.6) (�15.8) 84.0%
P � 0.16
Movement time (MT) 427 ms 403 ms 24 ms 418 ms 426 ms 8 ms
(�37.5) (�30.2) 95.7% (�32.6) (�39.1) 81.9%
P � 0.18
* Asterisk indicates a significant difference from the pre-test condition. Significant differences were detected in the pre- to posttest differences between control and stretch conditions
for balance (power: �50%), RT (power: �95%), and MT (power: �50%).
STRETCHING EFFECTS ON BALANCE AND MOVEMENT Medicine & Science in Sports & Exercise� 1399
moderate-large) and movement (P � 0.01, effect size �
0.65: moderate) time, respectively (Table 1). In reference to
the pretest control session, RT and MT improved (decreased)
by 5.8% (P � 0.16) and 5.7% (P � 0.18), respectively.
However, compared to the pretest stretch condition,
RT and MT were impaired (increased) by 4.0% and 1.9%
poststretch, respectively (nonsignificant).
DISCUSSION
The most important findings in this study were the impairments
in balance, RT and MT, due to prior stretching.
The control condition which involved a 5-min cycle warmup,
submaximal and maximal leg extension contractions,
three trials each of rapid leg movement (RT and MT), and
balance on a wobble board followed by a 26 min rest period
improved performance in the balance, RT and MT tests.
Inserting a stretching routine within the rest period not only
nullified the beneficial effects of the warm-up but also
produced small performance decrements in relation to the
pretest scores.
These decrements reflect impairments associated with
recent studies that have reported stretch-induced decreases
in force (4,13,14), power (11,40), and muscle activation
(2,4,13). Although isometric forces decreased 6.9% after
stretching in the present study, the decrement was not significantly
greater than the 5.6% impairment in the control
condition. The lack of a significant loss of isometric force
may be attributed to the moderate volume of stretching
imposed. In contrast to other similar studies that have
stretched a single muscle group for 15–30 min (4,13,14), the
present study involved only 135 s of intermittent stretching
for each of the three muscle groups.
Balance involves the interaction of automatic postural
and voluntary motor commands of both the trunk and limb
musculature (6,30). Balancing on a wobble board can involve
unanticipated perturbations to equilibrium that are
adjusted through contractions of both trunk and limb muscles.
Bloem and colleagues (6) speculated that lower leg
inputs act to modulate automatic postural responses. They
also found that the knees, hips, and trunk initiated movement
before the automatic postural responses. The CNS
performs anticipatory postural adjustments when expecting
self-inflicted postural perturbations (1). However, Aruin and
colleagues (1) suggested that under conditions of high instability
that the CNS may suppress anticipatory postural
adjustments as protection against their possible destabilizing
effects. Consequently, voluntary responses of trunk and
limb muscles to postural challenges would play a prominent
role. Shiratori and Latash (30) in a subsequent study from
the same laboratory reported that distal muscles (tibialis
anterior and soleus) cope with asymmetrical perturbations
and modulate the anticipatory postural adjustments in novel
situations (i.e., wobble board). Furthermore, Lipshits et al.
(22) described how perturbing balance by rapidly raising a
hand was initially counteracted by activation of lower limb
muscles. Therefore, it is apparent the important role that
lower limbs play in maintaining balance. Modifications to
either the afferent limb muscle responses or the mechanical
output would be expected to affect the ability of the peripheral
neuromuscular system to adapt effectively to stability
challenges.
Stretching has been reported to alter the length and stiffness
of the affected limb MTU. Although the exact mechanisms
responsible for increases in range of motion after
stretching are debatable, the increase is commonly attributed
to decreased MTU stiffness (37,39). Fowles et al. (13)
demonstrated an 8-mm increase in fascicle length of the
soleus and lateral gastrocnemius with 30 min of stretching.
Studies have reported both decreases (24,35) and no change
(23) in MTU passive resistance or stiffness with stretching.
Changes in MTU stiffness might be expected to affect the
transmission of forces, the rate of force transmission and the
rate at which changes in muscle length or tension are detected.
A more slack parallel and series elastic component
could increase the electromechanical delay by slowing the
period between myofilament crossbridge kinetics and the
exertion of tension by the MTU on the skeletal system. In
addition, the detection and monitoring of the muscle tension
by the Golgi tendon organs (GTO) would be delayed since
a more compliant tendon would not transmit the tension
information to the GTO as rapidly as a stiffer MTU. Furthermore,
increases in MTU length and decreases in MTU
stiffness could also alter the perception of the intrafusal
stretch receptors and thus perturb the afferent responses to
both changes in muscle length, rate of length change, and
tension (GTO). Therefore, stretch-induced changes in muscle
compliance might affect both the muscle afferent input
to the CNS and muscle output for counteracting unexpected
perturbations to balance.
Further evidence for the detrimental effect of an acute
bout of stretching on the CNS has been provided by Avela
et al. (2). They investigated the effects of passive stretching
of the triceps surae muscle on reflex sensitivity. After 1 h of
stretching, there were significant decreases in MVC
(23.2%), EMG (19.9%), stretch reflex peak-to-peak amplitude
(84.8%), and the ratio of H-reflex to muscle compound
action potential (M-wave) (43.8%). Although neural propagation
seemed unaffected (M-wave), afferent excitation of
the motoneuron pool (H-reflex) was impaired. They suggested
that the decrease in the excitation of the motoneuron
pool resulted from a reduction in excitatory drive from the
Ia afferents onto the �-motoneurons, possibly due to decreased
resting discharge of the muscle spindles via increased
compliance of the MTU.
Stretch-induced impairments in RT and MT may be related
to similar mechanisms as the disturbance in balance.
As mentioned previously, a more compliant MTU could
compromise the rate of tension development. Although it is
highly unlikely that the visual detection of the light stimulus
and the subsequent initiation of CNS motor programs to
move the leg would be adversely affected by stretching, a
prolonged electromechanical delay could negatively affect
both RT and MT. Although not monitored in the present
study, other studies have reported decreases in muscle activation
after stretching (2,4,13). Increases in motoneuron
1400 Official Journal of the American College of Sports Medicine http://www.acsm-msse.org
inhibition are more likely to affect the high-threshold fastcontracting
motor units that could also play a role in stretchinduced
RT and MT impairments.
An interesting development in the present study was the
control condition’s improvements in balance scores, RT and
MT. This finding may provide support for the beneficial
effect of a short duration, combination of general (cycle
warm-up and leg extension contractions) and specific (pretest
wobble board, RT and MT tests) activities. However,
because there was no condition in which a cycle warm-up
was not included, the contribution of the cycling cannot be
precisely deduced from the present study.
Young and Behm (41) reported similar results in a study
where subjects participated in five different warm-ups in a
randomized order before the performance of two jumping
tests. The warm-ups were: a) control, b) 4-min run, c) static
stretch, d) run and static stretch, and e) run and static stretch
and practice jumps. Generally, the stretching warm-up produced
the lowest values and the run or run and stretch and
jumps warm-ups produced the highest values of explosive
force production. Thus, it should not be surprising that the
control condition’s dynamic warm-up and static leg extension
contractions facilitated subsequent performance.
Numerous studies have investigated the effects of actively
warming-up on subsequent performance, yielding
mixed results. Although the majority of the research has
demonstrated that an increase in temperature facilitates human
performance (9,29,32), other studies have shown inhibitory
effects (5,16) as well as no effect (7) of warming-up
on subsequent performance. These conflicting results may
be attributed to discrepancies in the type of exercise, intensity,
duration, or any combination of these variables utilized
in the warm-up procedure. Studies have demonstrated that
warming-up can result in increased nerve conduction velocity
(31). Increases in nerve conduction velocity could facilitate
the response speed to perturbation in balance as well as
contributing to the improvements in RT and MT.
Another mechanism that may help explain the control
condition’s improvement in RT, MT, and balance may be
the effect of postactivation potentiation (PAP). PAP can be
defined as an increase in the efficiency of the muscle to
produce submaximal force after a voluntary contraction.
PAP has been attributed to regulatory light chain (RLC)
phosphorylation (17,20,21,33), which increases the number
of force-producing crossbridges under conditions of suboptimal
Ca2� activation (33). Suboptimal Ca2� activation may
be present with lower-frequency stimulation such as the
lower-intensity contractions associated with static balance.
Potentiation also involves an increase in the rate constant of
crossbridge attachment (20). The increased rate constant
would allow a greater number of crossbridges to form during
a specific time period resulting in increased force and
rate of force development capabilities. Furthermore, at the
supraspinal level, motor-evoked potential facilitation has
been reported after different durations (5, 15, and 30 s) and
intensities (10%, 25%, and 50%) of thenar muscle voluntary
contractions (3). A number of studies have suggested that an
improved neuromuscular activation can occur after a few
MVC (18,40). Evidence of this postcontraction neural potentiation
is provided by increased H-reflex amplitudes (18)
that may persist for 10 min after the contractions (36). Thus,
pretest contractions in the control condition may have elicited
a PAP response providing both a facilitation of the
motoneuron excitation and RLC phosphorylation contributing
to the significant improvements in RT and MT. Indirectly,
the PAP-induced augmentation of RT and MT would
also benefit balance by allowing more rapid responses to the
perturbations of the unstable environment. The stretching
condition may have nullified the beneficial effects of PAP
contributing to the 2.2% decrement in balance scores.
ICC (reliability) for the dependent measures were all in
the good to excellent category (0.80–0.93) except for the
day-to-day reliability of RT that scored 0.60 (moderate). A
paired samples t-test was then conducted on the RT measures.
The lack of significant difference between the measures
suggested that the low RT ICC may be attributed to the
low between subject variability. Another contributing factor
for this less than optimal reliability may be due to the test
set-up. The RT test for the lower limb necessitated that the
individuals place most of their mass on the nondominant
limb creating a degree of instability. Even with an orientation
session, the lack of familiarity with this type of movement
and the greater instability may have led to a less
consistent action.
CONCLUSION
In summary, the findings of the present study demonstrate
that a moderate bout of stretching (three repetitions per
muscle group) held to the point of discomfort can adversely
affect performance on tests of static balance, RT and MT.
The stretch-induced impairments are hypothesized to be
related to changes in muscle compliance with the stretching
that may adversely affect the ability to detect and respond to
changes in muscle length, and rate of change in muscle
length and forces. Furthermore, it was found in the present
study that a warm-up consisting of general and specific
activities related to the tasks may improve performance
even after 20 min of recovery. Considering the minute
differences between winning and losing in both individual
and team sports as well as the precarious balance or stability
of the elderly, the low but significant percentage changes in
RT, MT, and balance could result in serious consequences.
REFERENCES
1. ARUIN, A. S., W. R. FORREST, and M. L. LATASH. Anticipatory
postural adjustments in conditions of postural instability. Electroencephal.
Clin. Neurophysiol. 109:350–359, 1998.
2. AVELA, J., H. KYR¨OL¨AINEN, and P. V. KOMI. Altered reflex sensitivity
after repeated and prolonged passive muscle stretching.
J. Appl. Physiol. 86:1283–1291, 1999.
STRETCHING EFFECTS ON BALANCE AND MOVEMENT Medicine & Science in Sports & Exercise� 1401
3. BALBI, P., A. PERRETTI, M. SANNINO, L. MARCANTONIO, and L.
SANTORO. Post-exercise facilitation of motor evoked potentials
following transcranial magnetic stimulation: a study in normal
subjects. Muscle Nerve 25:448–452, 2002.
4. BEHM, D. G., D. BUTTON, and J. BUTT. Factors affecting force loss
with stretching. Can. J. Appl. Physiol. 26:262–272, 2001.
5. BISHOP, D., D. BONETTI, and B. DAWSON. The effect of three
different warm-up intensities on kayak ergometer performance.
Med. Sci. Sports Exerc. 33:1026–1032, 2001.
6. BLOEM, B. R., J. H. J. ALLUM, M. G. CARPENTER, and F. HONEGGER.
Is lower leg proprioception essential for triggering human automatic
postural responses? Exp. Brain Res. 130:375–391, 2000.
7. BRUYN-PREVOST, P. The effect of various warming-up intensities
and durations upon some physiological variables during an exercise
corresponding to PWC 170. Eur. J. Appl. Physiol. 43:93–100,
1980.
8. BURKE, D. Muscle spindle function during movement. In: The
Motor System in Neurobiology, E. V. Evarts, S. P. Wise, and D.
Bousfield (Eds.). New York: Elsevier Biomedical Press, 1985, pp.
168–172.
9. CHWALBINSKA-MONETA, J., and O. HANNINEN. Effects of active
warming-up on thermoregulatory, circulatory, and metabolic responses
to incremental exercise in endurance trained athletes. Int.
J. Sport Med. 10:25–29, 1989.
10. COOKE, J. D. The role of stretch reflexes during active movements.
Brain Res. 181:493–497, 1980.
11. CORNWELL, A., A. G. NELSON, and B. SIDAWAY. Acute effects of
stretching on the neuromechanical properties of the triceps surae
muscle complex. Eur. J. Appl. Physiol. 86:428–434, 2002.
12. FERBER, R., L. R. OSTERNIG, and D. GRAVELLE. Effect of PNF
stretch techniques on knee flexor muscle EMG activity in older
adults. J. Electromyogr. Kinesiol. 12:391–397, 2002.
13. FOWLES, J. R., D. SALE, and J. D. MACDOUGALL. Reduced strength
after passive stretch of human plantar flexors. J. Appl. Physiol.
89:1179–1188, 2000.
14. FOWLES, J. R., and D. G. SALE. Time course of strength deficit after
maximal passive stretch in humans. Med. Sci. Sports Exerc. 29:
S26, 1997.
15. FOWLES, J. R., D. G. SALE, and J. D. MACDOUGALL. Reduced
strength after passive stretch of the human plantar flexors. J. Appl.
Physiol. 89:1179–1188, 2000.
16. GENOVELY, H., and B. A. STAMFORD. Effects of prolonged warm-up
exercise above and below the anaerobic threshold on maximal
performance. Eur. J. Appl. Physiol. 48:232–330, 1982.
17. GRANGE, R. W., R. VANDENBOOM, and M. E. HOUSTON. Physiological
significance of myosin phosphorylation in skeletal muscle.
Can J. Appl. Physiol. 18:229–242, 1993.
18. GULLICH, A., and D. SCHMIDTBLEICHER. MVC-induced short-term
potentiation of explosive force. New Studies in Athletics 11:67–
81, 1996.
19. HARVEY, L., R. HERBERT, and J. CROSBIE. Does stretching induce
lasting increases in ROM? A systematic review. Physiotherapy
Res. Intern. 7:1–13, 2002.
20. HOUSTON, M. E., and R. W. GRANGE. Myosin phosphorylation,
twitch potentiation, and fatigue in human skeletal muscle. Can
J. Physiol. Pharm. 68:908–913, 1990.
21. HOUSTON, M. E., H. J. GREEN, and J. T. STULL. Myosin light chain
phosphorylation and isometric twitch potentiation in intact human
muscle. Pflu¨gers Arch. Eur. J. Physiol. 403:348–352, 1985.
22. LIPSHITS,M. I., K.MAURITZ, and K. E. POPOV. Quantitative analysis
of anticipatory postural components of a complex voluntary movement.
Fiziologiya Cheloveka 7:411–419, 1982.
23. MAGNUSSON, S. P., P. AAGAARD, and J. J. NIELSEN. Passive energy
return after repeated stretches of the hamstring muscle tendon unit.
Med. Sci. Sports Exerc. 32:1160–1164, 2000.
24. MAGNUSSON, S. P., E. B. SIMONSEN, P. AAGAARD, and M. KJAER.
Biomechanical responses to repeated stretches in human hamstring
muscle in vivo. Am. J. Sports Med. 24:622–627, 1996.
25. MCGRAW, K. O., and S. P. WONG. Forming inferences about some
intraclass correlation coefficients. Psychol. Methods 1:30–46,
1996.
26. NASHNER, L. M. Adapting reflexes controlling the human posture.
Exp. Brain Res. 26:59–72, 1976.
27. NELSON, M. E., M. A. FIATORONE, C. M. MORGANTI, I. TRICE, R. A.
GREENBERG, and W. J. EVANS. Effects of high intensity strength
training on multiple risk factors for osteoporotic fractures: a randomized
control trial. JAMA 272:1909–1914, 1994.
28. POLIDORO, J. R. Sport and Physical Activity in the Modern World.
Needham Heights, MA: Allyn and Bacon, 2000, pp. 124–132.
29. ROBERGS, R. A., D. D. PASCOE, D. L. COSTILL, et al. Effects of
warm-up on muscle glycogenolysis during intense exercise. Med.
Sci. Sports Exerc. 23:37–43, 1991.
30. SHIRATORI, T., and M. LATASH. The roles of proximal and distal
muscles in anticipatory postural adjustments under asymmetrical
perturbations and during standing on rollerskates. Clin. Neurophysiol.
111:613–623, 2000.
31. STEGMAN, D. F., and J. P. DE WEERD. Modelling compound action
potentials of peripheral nerves in situ. II. A study of the influence
of temperature. Electroencephal. Clin. Neurophysiol. 54:516–529,
1982.
32. STEWART, I. B., and G. G. SLIEVERT. The effect of warm-up intensity
on range of motion and anaerobic performance. J. Orthop.
Sports Phys. Therapy 27:154–161, 1998.
33. SWEENEY, H. L., B. F. BOWMAN, and J. T. STULL. Myosin light chain
phosphorylation in vertebrate striated muscle: regulation and function.
Am. J. Physiol. (Cell Physiol.) 264:c1085–c1095, 1993.
34. TAYLOR, D. C., J. D. DALTON, A. V. SEABER, and W. E. GARRET.
Viscoelastic properties of muscle-tendon units: the biomechanical
effects of stretching. Am. J. Sports Med. 18:300–308, 1990.
35. TOFT, E., G. T. ESPERSEN, S. KåLUND, T. SINKJÆR, and B. C.
HORNEMANN. Passive tension of the ankle before and after stretching.
Am. J. Sports Med. 17:489–494, 1989.
36. TRIMBLE, M. H., and S. S. HARP. Postexercise potentiation of the
H-reflex in humans. Med. Sci. Sports Exerc. 30:933–941, 1998.
37. WILSON, G., B. ELLIOT, and G. WOOD. Stretching shorten cycle
performance enhancement through flexibility training. Med. Sci.
Sports Exerc. 24:116–123, 1992.
38. WILSON, G. J., A. MURPHY, and J. F. PRYOR. Musculotendinous
stiffness: its relationship to eccentric, isometric and concentric
performance. J. Appl. Physiol. 76:2714–2719, 1994.
39. WILSON, G. J., G. A. WOOD, and B. C. ELLIOT. The relationship
between stiffness of the musculature and static flexibility: an
alternative explanation for the occurrence of muscular injury.
Intern. J. Sports Med. 12:403–407, 1991.
40. YOUNG, W., and J. ELLIOTT. Acute effects on static stretching,
proprioceptive neuromuscular facilitation stretching, and maximum
voluntary contractions on explosive force production and
jumping performance. Res. Q. Exerc. Sport 72:273–279, 2001.
41. YOUNG, W. B., and D. G. BEHM. Effects of running, static stretching
and practice jumps on explosive force production and jumping
performance. J. Sport Med. Phys. Fitness 34: 119–124, 2003.
1402

 Slipped disk: A slipped disk is also called a herniated disc. Normally, disks in your spine provide space and cushioning between the bones in your spine. A slipped disk occurs when part of the much softer disk bulges out and pushes against nearby nerves. This causes severe pain and discomfort, as well as radiating pain symptoms down your legs or arms. Most cases of slipped discs heal over time, with the aid of physical therapy. ONLY most severe cases might need surgery.
Slipped disk: A slipped disk is also called a herniated disc. Normally, disks in your spine provide space and cushioning between the bones in your spine. A slipped disk occurs when part of the much softer disk bulges out and pushes against nearby nerves. This causes severe pain and discomfort, as well as radiating pain symptoms down your legs or arms. Most cases of slipped discs heal over time, with the aid of physical therapy. ONLY most severe cases might need surgery.

 Teeth grinding can be the cause of different symptoms which include facial pain, migraines, headaches, ear-ache, tightness and stiffness in the shoulders, pain and stiffness in the jaw joint, abnormal tooth wear and restless or disrupted sleep.
Teeth grinding can be the cause of different symptoms which include facial pain, migraines, headaches, ear-ache, tightness and stiffness in the shoulders, pain and stiffness in the jaw joint, abnormal tooth wear and restless or disrupted sleep.
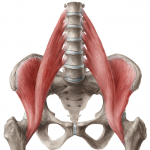 Regardless of the nature of the pain and how it makes you feel, one primary muscle that is involved in causing back pain is the Psoas, or perhaps more accurately – the
Regardless of the nature of the pain and how it makes you feel, one primary muscle that is involved in causing back pain is the Psoas, or perhaps more accurately – the 